- 1. What Is Luteal Phase Defect?
- 2. Why Luteal Phase Defect Is Often Missed
- 3. Common Signs of Luteal Phase Defect
- 3.1. 1. Short Luteal Phase
- 3.2. 2. Spotting Before Your Period
- 3.3. 3. PMS That Feels Intense or Sudden
- 3.4. 4. Trouble Maintaining Early Pregnancy
- 3.5. 5. Poor Sleep in the Second Half of the Cycle
- 4. What Causes Luteal Phase Defect?
- 4.1. Hormonal & Physiological Factors
- 4.2. Lifestyle & Metabolic Factors
- 5. How Luteal Phase Defect Affects Fertility
- 6. How Luteal Phase Defect Is Identified
- 7. Supporting a Healthy Luteal Phase (Educational Insight)
- 8. Why Understanding Luteal Phase Defect Matters
If you’ve ever felt like you’re “doing everything right” but your cycle still feels off, you’re not alone. One of the most commonly overlooked hormone-related issues in women is luteal phase defect—a condition that quietly affects cycle regularity, hormonal balance, and fertility potential.
What makes luteal phase defect so frustrating is that periods can still arrive every month, ovulation tests may turn positive, and yet something still doesn’t feel quite right. This guide breaks down what luteal phase defect really is, how it shows up, and why so many women don’t realize it’s happening.
Luteal Phase Defect The Silent Hormone Issue That Can Disrupt Your Cycle Fertiease
What Is Luteal Phase Defect?
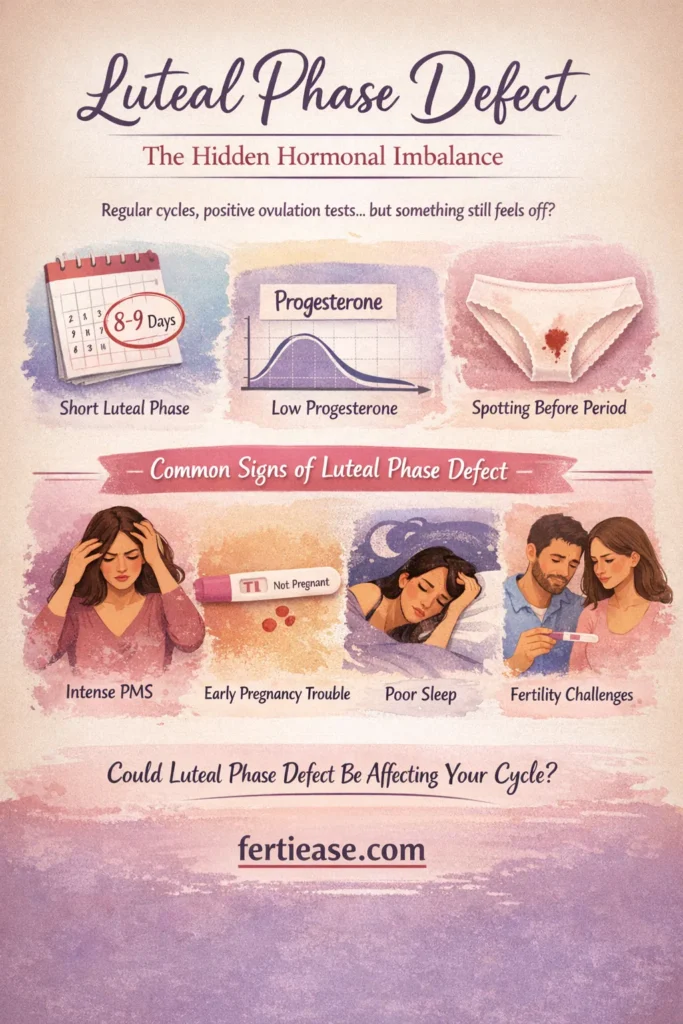
The luteal phase is the second half of your menstrual cycle—the time between ovulation and your next period. In a healthy cycle, this phase lasts 12–14 days and is dominated by the hormone progesterone.
")
Luteal phase defect occurs when:
the luteal phase is consistently too short (usually under 10 days), or
progesterone levels are too low to properly support the cycle
When this happens, the uterine lining may not be fully prepared, hormones fluctuate more sharply, and the cycle becomes less stable—even if ovulation technically occurs.
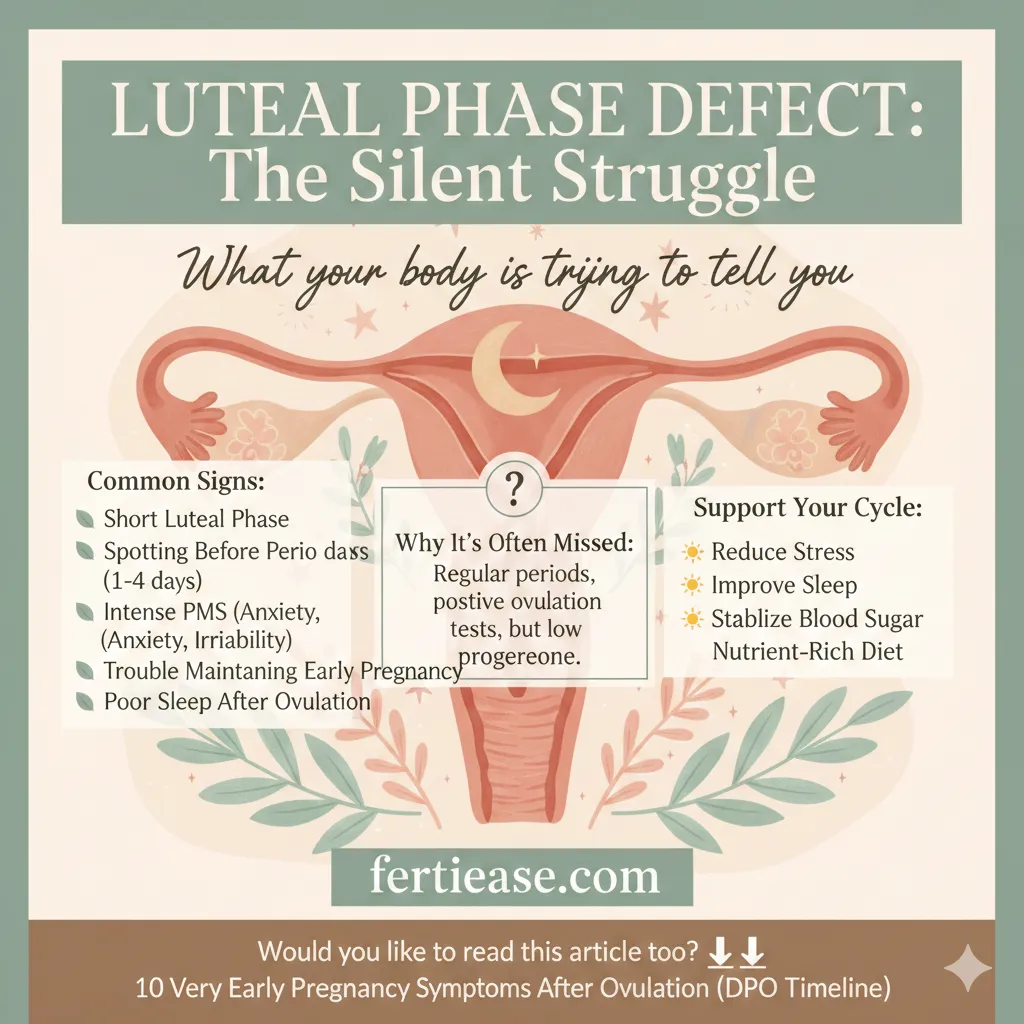
Why Luteal Phase Defect Is Often Missed
One reason luteal phase defect goes unnoticed is because:
periods still come regularly
cycles may still be 26–30 days long
ovulation kits may still show an LH surge
But beneath the surface, progesterone may not be rising high enough—or staying elevated long enough—to support a healthy luteal phase.
Many women only discover luteal phase defect after months of tracking, unexplained PMS, or difficulty conceiving.
Common Signs of Luteal Phase Defect
Luteal phase defect doesn’t always come with dramatic symptoms. Instead, it shows up in subtle but recurring patterns.
1. Short Luteal Phase
If you track ovulation and your period consistently starts 8–10 days later, this is one of the strongest signs of luteal phase defect.
2. Spotting Before Your Period
Light spotting 1–4 days before full bleeding often indicates progesterone is dropping too early.
3. PMS That Feels Intense or Sudden
Low progesterone can amplify:
anxiety
irritability
breast tenderness
sleep disturbances
emotional sensitivity
Symptoms may appear quickly and feel disproportionate to the rest of the cycle.
4. Trouble Maintaining Early Pregnancy
Progesterone plays a critical role in supporting early implantation. When levels are insufficient, implantation may be unstable—even before a missed period.
Luteal Phase Defect The Silent Hormone Issue That Can Disrupt Your Cycle 2 Fertiease
5. Poor Sleep in the Second Half of the Cycle
Waking up during the night, restless sleep, or early-morning anxiety after ovulation is a common but under-recognized sign.
What Causes Luteal Phase Defect?
There is rarely a single cause. Most cases involve a combination of hormonal and lifestyle factors.
Hormonal & Physiological Factors
low progesterone production
weak ovulation
thyroid imbalance
elevated prolactin
estrogen dominance
Lifestyle & Metabolic Factors
chronic stress (high cortisol suppresses progesterone)
under-eating or over-exercising
blood sugar instability
poor sleep
rapid weight changes
Even women with “normal” labs can experience luteal phase defect if the hormonal rhythm is disrupted.
How Luteal Phase Defect Affects Fertility
Luteal phase defect doesn’t always prevent pregnancy, but it can make conception more challenging by:
shortening the implantation window
reducing uterine lining stability
increasing early cycle hormone fluctuations
making timing less predictable
For women trying to conceive, addressing luteal phase health is often just as important as confirming ovulation.
How Luteal Phase Defect Is Identified
There is no single test that diagnoses luteal phase defect on its own. Instead, it’s identified through patterns such as:
consistent short luteal phases
progesterone testing about 7 days after ovulation
basal body temperature charts that drop early
repeated premenstrual spotting
Tracking over multiple cycles provides the clearest picture.
Supporting a Healthy Luteal Phase (Educational Insight)
While treatment decisions should always be made with a healthcare professional, many women are encouraged to focus on:
reducing chronic stress
supporting sleep quality
stabilizing blood sugar
avoiding excessive exercise during the luteal phase
ensuring adequate caloric intake
improving overall hormonal rhythm
The goal is to help progesterone rise naturally and remain stable through the second half of the cycle.
Why Understanding Luteal Phase Defect Matters
Luteal phase defect is not rare—and it’s not a personal failure or something you “missed.” It’s a sign that your body may need better hormonal support, not more pressure or stricter control.
Understanding this condition helps many women finally make sense of:
persistent PMS
unexplained cycle irregularities
feeling “off” after ovulation
fertility frustration despite regular cycles
Your cycle is a conversation your body is having with you. Luteal phase defect is one way it asks for attention.
Would you like to read this article too? ⬇️⬇️
10 Very Early Pregnancy Symptoms After Ovulation (DPO Timeline)
What is your reaction to this article?
Here is a professional English bio for Dr. Elizabeth Williams, Obstetrician-Gynecologist: Dr. Elizabeth Williams, MD, FACOG, is a board-certified obstetrician-gynecologist with over 15 years of experience providing compassionate, evidence-based women’s healthcare. She earned her medical degree from Johns Hopkins University School of Medicine and completed her residency in Obstetrics and Gynecology at Massachusetts General Hospital, Harvard Medical School, where she served as Chief Resident. Dr. Williams specializes in high-risk pregnancies, minimally invasive gynecologic surgery, adolescent gynecology, and menopause management. Known for her warm bedside manner and clear communication, she is dedicated to empowering her patients through every stage of life, from prenatal care and childbirth to preventive wellness and complex gynecologic conditions. In addition to her clinical practice, Dr. Williams is actively involved in medical education and has published research on preeclampsia, labor induction, and robotic-assisted surgery. She is a Fellow of the American College of Obstetricians and Gynecologists (FACOG) and a member of the Society for Maternal-Fetal Medicine. Patients describe Dr. Williams as “attentive, knowledgeable, and truly caring,” and she is proud to deliver hundreds of babies each year while building long-term relationships with the families she serves. Dr. Williams practices in [City/State] and is affiliated with [Hospital Name]. She welcomes new patients and offers both in-person and telemedicine appointments.
VIEW AUTHOR PROFILE